“四踝”骨折的内固定方式与固定顺序
时间:2021-11-04 18:01:45 热度:37.1℃ 作者:网络

研究者提出了一种固定三踝骨折同时伴有胫骨前结节(“四踝”)或腓骨前缘(“类四踝”)骨折的新技术。24例患者平均年龄60岁,均采用切开复位内固定治疗。四踝骨折17例,类四踝骨折骨折6例。一名患者除三踝骨折外,合并胫骨前部和腓骨撕脱骨折。
20例采用俯卧位后踝直接切开复位内固定术,4例采用仰卧位后踝前后螺钉内固定术。所有四踝骨折固定后,术中检查时只有1例(4%)患者需要下胫腓联合螺钉治疗韧带联合不稳定。没有感染及伤口愈合问题。
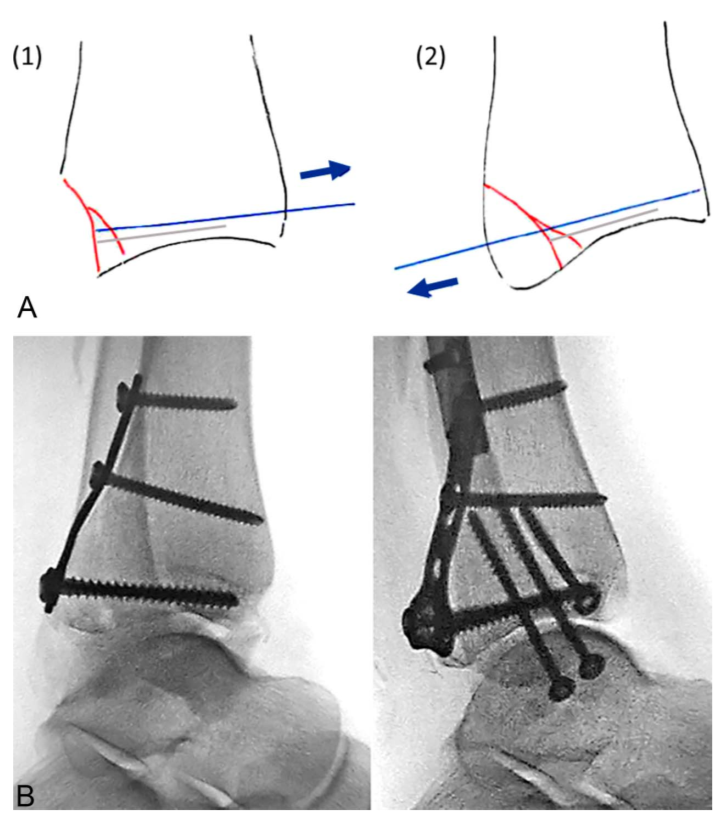
所有病人都进行了牢固的固定。19名患者(79%)接受了平均77个月的随访(范围15-156个月)。足部功能指数平均为15(范围50-0),Olerud-Molander评分平均为79(范围,45-100),AOFAS后足评分平均为87(范围,39-100)。通过提供骨对骨的固定,前、后胫骨碎片的固定增加了下胫腓联合的稳定性。胫骨前后缘的解剖复位恢复了胫骨切缘的生理形状,因此有利于腓骨复位。[Summary: We present a technique of fixation of trimalleolar fractures with additional fracture of the anterior tibial tubercle (“quadrimalleolar”) or anterior fibular rim (“quadrimalleolar equivalent”). Twenty-four patients with a mean age of 60 years were treated with open reduction and internal fixation of all 4 malleoli. There were 17 quadrimalleolar and 6 quadrimalleolar equivalent fractures. One patient had both anterior tibial and fibular avulsion fracture in addition to a trimalleolar ankle fracture. Surgical approaches and internal fixation were tailored individually. Twenty patients were operated in the prone position with direct ixation of the posterior malleolus and 4 patients in the supine position with anterior to posterior screw fixation of the posterior malleolus. After fixation of al 4 malleoli, only 1 patient (4%) required a syndesmotic screw for residual syndesmotic instability on intraoperative testing. There were no infections and no wound healing problems. All patients went on to solid union. Nineteen patients (79%) were followed for a mean of 77 months (range, 15–156 months). The Foot Function Index averaged 15 (range, 50 to 0), the Olerud and Molander Score averaged 79 (range, 45–100), and the American Orthopaedic Foot and Ankle Society Ankle and Hindfoot Scale averaged 87 (range, 39–100). Fixation of the anterior and posterior tibial fragments increases syndesmotic stability by providing a bone-to-bone fixation. Anatomic reduction of the anterior and posterior tibial rim restores the physiological shape of the tibial incisura and therefore facilitates fibular reduction.]
Surgical technique(手术技术)
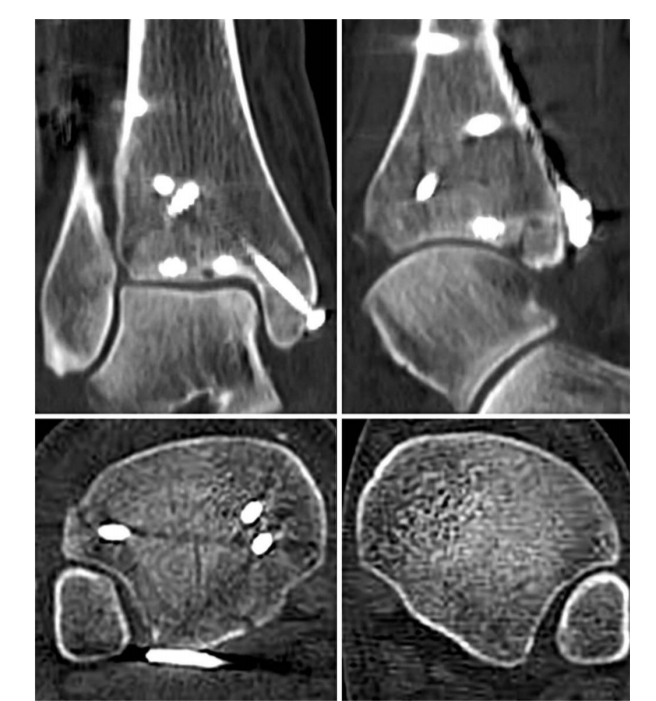
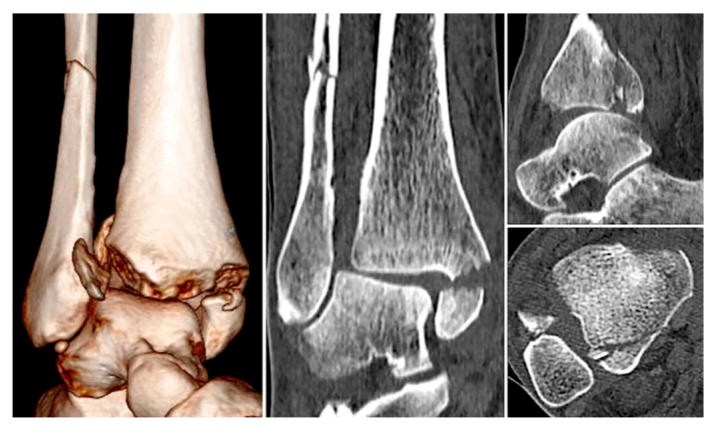
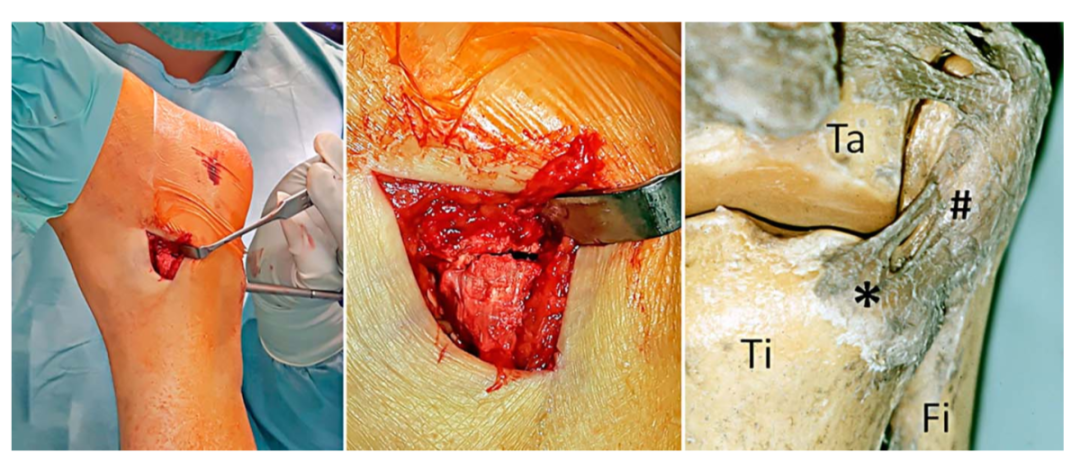
① 四踝骨折示意图:1.内踝;2.外踝;3.后踝;4.胫骨前结节(前踝)。 ② 四踝骨折典型病例图。
② 四踝骨折典型病例图。
 ③首先俯卧位后外侧入路固定后踝,存在夹层骨块可行克氏针临时固定后抗滑钢板固定后踝。
③首先俯卧位后外侧入路固定后踝,存在夹层骨块可行克氏针临时固定后抗滑钢板固定后踝。
 ④ 固定后踝后,经同一后外侧切口固定外踝,通常建议采用后侧钢板固定,如腓骨骨折线过高,则重新切口外侧钢板固定腓骨。
⑤ 内踝常规切口固定内踝。
⑥ 俯卧位患者屈曲膝关节,经前外侧切口固定前踝骨折块,通常选用2.7mm或3.5mm螺钉,并使用垫圈。
④ 固定后踝后,经同一后外侧切口固定外踝,通常建议采用后侧钢板固定,如腓骨骨折线过高,则重新切口外侧钢板固定腓骨。
⑤ 内踝常规切口固定内踝。
⑥ 俯卧位患者屈曲膝关节,经前外侧切口固定前踝骨折块,通常选用2.7mm或3.5mm螺钉,并使用垫圈。
⑦ 固定后常规检查下胫腓联合稳定性。